

What happens if Colorado hospitals have to start choosing who gets a hospital bed?

Here’s a nightmare scenario.
In the wake of Thanksgiving, COVID rates spike even higher. Hospitalizations climb higher than their record-setting peaks. Health care workers keep getting sick. Hospitals stretch and then lose their capacity to treat all the patients – COVID or not – walking through their doors. Transferring patients to other facilities is drastically limited or blocked completely. All the while, the sick and injured keep coming.
Should hospitals become overwhelmed, the state will enact a plan drawn up in April to ration care to the most likely to survive. The crisis standards of care will lay out a blueprint by which hospitals will use to give individual patients a score from one to eight, with eight being the worst. It will determine whose families get a phone call saying that there aren’t enough beds or staff to keep your loved one alive.
The better scores will receive life-saving care that, under this yet-to-be-realized, worst-case scenario, must now be rationed. Those with poorer scores, determined by their likelihood to survive immediately and for the next year, will be made comfortable and given what care is available as they die.
“This is the future we’ll have should we fail to prevent more spread,” said Matt Wynia, a doctor and the head of the Center for Bioethics and Humanities at the University of Colorado’s Anschutz Medical Campus.
Officials have said that staffing problems represent a pressing threat to hospitals’ stability now; surge plans, both within facilities and at the state level, can produce more hospital beds and more space. But there’s a finite amount of staffing. More providers are getting sick, and there are few out-of-state reinforcements to bolster the exhausted ranks.
“The signs are pointing in the wrong direction,” Wynia said. “Partly because you think about all the things that have happened in the last couple of weeks, and what’s going to happen in the next week, namely Thanksgiving, and you just have to assume that this is not going to go away in the next couple of weeks.”
Most coronavirus data is lagging, and that delay is compounded the further you move down the chain of events. Speaking generally, it takes a week or two before you start to see new cases that were contracted today. It takes another week or two before you see that increase or decline reflected in hospitalizations, plus another two weeks before death rates go up or down. So actions taken today won’t alleviate any problem immediately, but the longer you wait, the longer the pain will be felt on the front lines.
The state drafted a crisis plan after the H1N1 pandemic in 2009. That plan is more broad, though it repeatedly alludes to a future pandemic. In the spring, as Colorado experts looked at horrors unfolding in Italy and New York, they decided to update those plans and build them around this pandemic.
At that time, officials were concerned that hospitals would run out of ventilators, said Anuj Mehta, a National Jewish physician who led the effort to draft the plan. That problem has largely fallen away and have been replaced by staffing and, as a necessary corollary, about bed capacity.
Still, the plan lays out how to assess patients and dole out limited resources should the worst happen. They describe the point system that a team of providers at each hospital – an administrator, a critical care physician, a nurse and an ethics or palliative care expert – would use to determine who will receive advanced care. This team will established a “cut” score: anyone above gets the treatment; anyone below doesn’t.
“Individuals would have to face the fact that, ‘Hey your dad went to the hospital, there was a way we could’ve treated him, and we didn’t have enough resources and couldn’t treat him,'” Mehta said. “And that’s just terrifying.”
The score is a combination of two grading systems. The first gives patients scores depending on their current status. It will assign them scores between one to four based on their breathing; their kidney, liver, nervous system and heart function; and their platelet count.
That score will be added to another that looks at patients’ near-term health, meaning their risk of dying in the next six to 12 months. That score looks at your age and your health history. Does the patient have AIDS? Does the patient have liver disease, dementia, heart failure? Is there kidney failure or a metastatic tumor? Mehta said officials would push for equity: Patients’ race and ethnicity would be excluded from the information provided to the care team, though the patient’s face is often included in medical records.
If patients have the same scores, the team will go down other tiers to break the tie. Is either patient a health care worker, a child, a first responder? If not, down to the next tier: Is the patient pregnant? How many years of life could be saved between one patient and another? Is the patient a caregiver or single parent?
If the scores are still tied, the decision will basically be made via coin flip, Mehta said.
When hospitals did “table reads” of the plan in the spring, it was traumatizing for providers, Mehta said.
“People were traumatized that they would have to make that decision about who gets a resource and who doesn’t,” he said. “I prayed I wouldn’t have to utter ‘crisis standards of care,’ and I’m very saddened we have to revisit this again. Every decision related to the crisis standards of care is tragic. Our goal, our primary goal is to save every patient in front of us.”
Both he and Wynia were up front with why they were willing to talk about it: They wanted Coloradans to know the worst-case scenario that’s inching closer to reality.
Wynia filled out the details of that nightmare.
Doctors and nurses would begin telling families, “Look, under normal circumstances, we would be moving your mom to the intensive care unit right now, but these are not normal circumstances, and we do not have beds in our intensive care unit, and we’re going to have to do the best we can, but it is very likely that your mom is going to die because of this illness.”
That mom, or daughter, or grandmother, or cousin, or coworker, or best friend would then be given palliative care, which in this case means end-of-life treatment. Ideally, hospitals will have enough room for that person to be in a hospital bed. But Wynia said that the patient could be moved to an overflow facility, such as the Colorado Convention Center (which has yet to be opened as a field hospital). Or they could be doubled up in a room with another patient. Or, in the worst-possible scenario in an already unimaginable moment, could be treated in a hallway.
There are specialists who focus on palliative care. They know how to talk to families and how to administer the proper medications. But Wynia said there are too few specialists to care for the number of patients who would need them in this situation, and he said there may not be enough narcotics to help them stay comfortable. Other medications – like the heavy-duty steroid given to President Donald Trump when he came down with the illness – would help COVID patients, but they may be reserved for those who scored higher.
Mehta said that intensive care specialists have enough palliative knowledge that they’d be able to help get those patients started.
“What the state is doing is setting up a palliative care hot line so doctors can call up and get better advice on how to treat patients who are dying,” Wynia said. “A hot line is not the same as having a sub-specialty trained physician. But that’s what we’re going to do because we’re going to have to do something when lots of people are dying and they need the best palliative care we can provide.”
In September, Wynia and two colleagues published a piece in the Journal of the American Medical Association warning about the shortage in palliative care experts. In it, they quoted a 2012 report that said that “the provision of palliative care in the context of a disaster with scarce resources can be considered a moral imperative of a humane society.”
As the patient dies, he or she may have limited visitation from family or loved ones. At the beginning of the pandemic, visitation for COVID patients specifically was fully blocked. Now, hospitals are loosening that because the idea of someone dying alone is “so terrifying and tragic,” Wynia said.
The last decision the hospital will make for a patient who’s been triaged comes after they die. Again, Wynia looks at the worst-case scenario elsewhere: mobile morgues, trucks parked outside of hospitals to handle an overflow of death.
Wynia said that health care workers are exhausted and he was concerned about adding the strains and horror that would come with the crisis plan.
“Can you imagine?” he said, referring to making triage calls when you’re already overworked and worn down.
“We’re not equipped mentally, as human beings,” to make these decisions, Metha said. “We care about our fellow people and our society, (and we aren’t equipped to say) ‘I’m going to give this resource to Person A and not Person B and that means Person B is going to die.'”
Both men stressed that it wasn’t too late. The nightmare can still be avoided, by wearing masks, by staying home, by not gathering, by having a limited Thanksgiving.


Energy secretary says U.S. must grow capacity, lower price during Colorado visit
Mark Samuelson Special to The Denver Gazette
mark.samuelson@denvergazette.com
Updated 8 hours ago
As a heatwave in the U.S. and Europe punctuated widespread calls for recommitments to solar and other “renewable” sources, U.S. Secretary of Energy Chris Wright doubled down on America’s current policy, telling a Thornton crowd on Monday that energy goals...
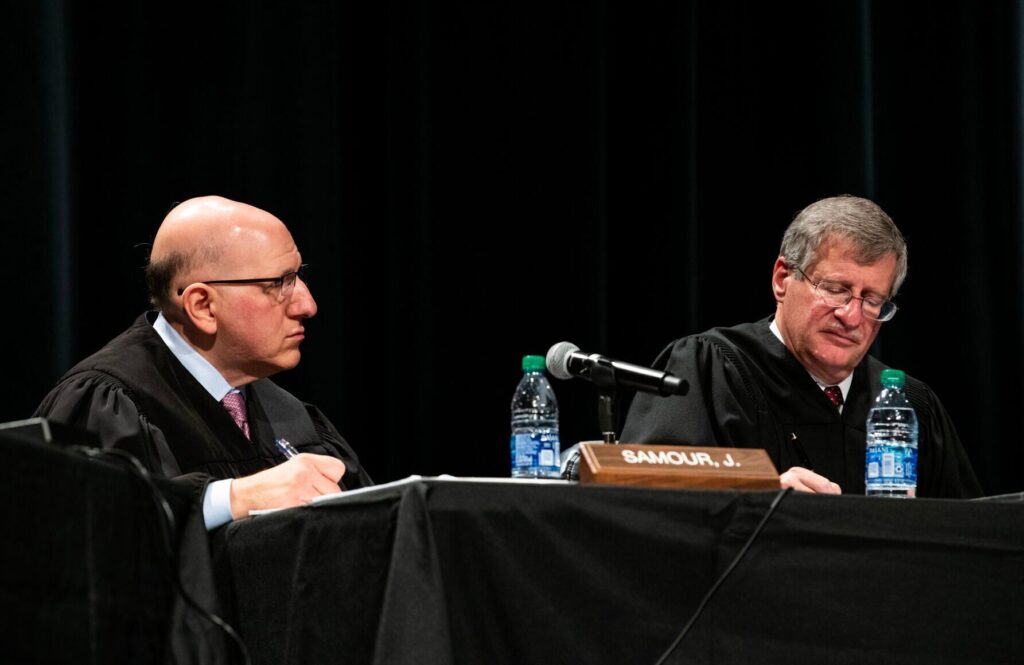
Colorado Supreme Court upholds child abuse convictions despite faulty jury instruction
Michael Karlik
michael.karlik@coloradopolitics.com
Updated 10 hours ago
The Colorado Supreme Court decided on Monday that a San Miguel County jury properly convicted a defendant of child abuse resulting in death, even though the instructions potentially allowed jurors to avoid finding that the child abuse resulted in death....

Gov. Polis asks residents not to use fireworks as wildfires burn
Rachael Wright, Special to Colorado Politics
rachael.wright@coloradopolitics.com
Updated 8 hours ago
While Gov. Jared Polis said he will not issue a statewide fire ban, Colorado’s top political leader urged residents against using fireworks as the country heads into the July 4 weekend. “We are encouraging the people of Colorado to exercise...

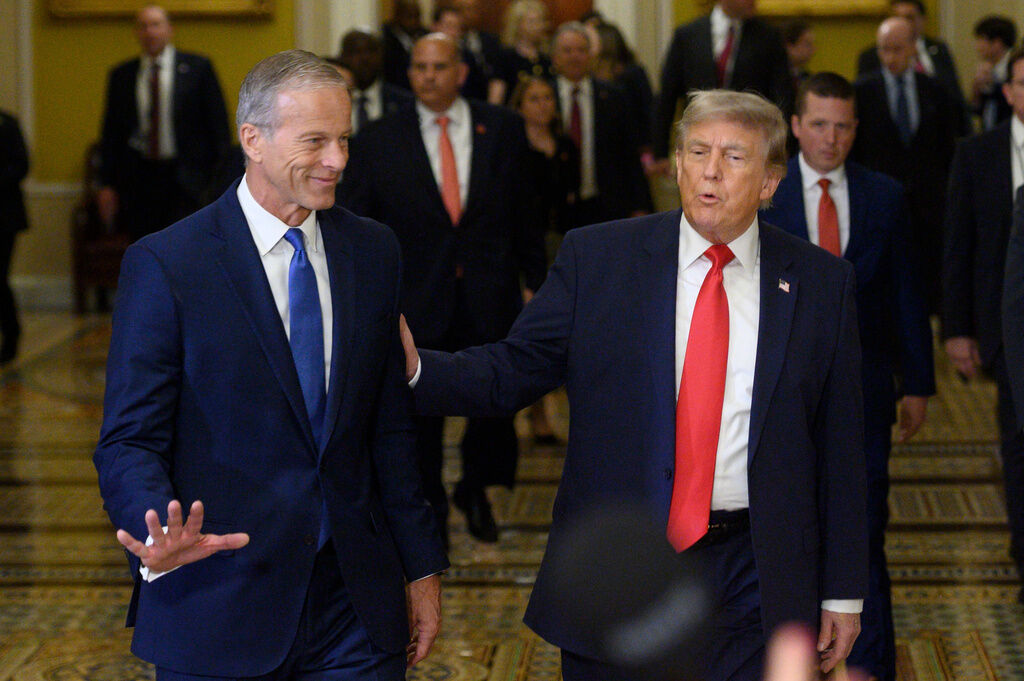
Trump says communism greater threat than WWI, WWII, 9/11, and Pearl Harbor
Naomi Lim
naomi-lim@coloradopolitics.com
Updated 11 hours ago
President Donald Trump compared the rise of socialism to the Sept. 11 terrorist attacks. Trump was asked about the possible rise of more socialist candidates after three candidates New York City Mayor Zohran Mamdani endorsed last week won their Democratic...
GOP doubles down on SAVE America Act after Supreme Court allows mail ballots to be counted late
Lauren Green
lauren-green@coloradopolitics.com
Updated 11 hours ago
Congressional Republicans continue to push the voter identification bill — that has left Washington in grid lock for months — after the Supreme Court ruled states can count mail-in ballots that arrive after Election Day. The 5-4 decision rejected a...

US and Iran to cease strikes and discuss Strait of Hormuz this week: Report
Carter Schroppe
carter.schroppe@washingtonexaminer.com
Updated 12 hours ago
Officials from the United States and Iran will meet in Qatar this week to discuss the Strait of Hormuz after agreeing to “halt strikes” following a weekend of intermittent fighting between the two countries. The meeting, scheduled for Tuesday in...

Congress is struggling to get its work done and a new report argues for 21st-century upgrades
Kevin R. Kosar
kevin-r-kosar@coloradopolitics.com
Updated 12 hours ago
The news coming from Capitol Hill over the past couple of weeks has left much to be desired. Congress has had difficulty discharging its lawmaking duties. The Senate’s appropriations committee is at loggerheads over how much spending to authorize. The...

Supreme Court rules constitutional privacy protections apply to cellphone users location history
The Associated Press
the-associated-press@coloradopolitics.com
Updated 13 hours ago
WASHINGTON (AP) — The Supreme Court held Monday that constitutional privacy protections extend to cellphone location information, ruling in the case of a bank robber whose identity was discovered through a geofence warrant. Justice Elena Kagan wrote for the 6-3...

Colorado justices say group that spent $4M on ballot initiatives does not have to disclose donors
Michael Karlik
michael.karlik@coloradopolitics.com
Updated 13 hours ago
The Colorado Supreme Court ruled on Monday that an organization that spent $4 million to advocate on ballot initiatives in the 2020 election is not required to disclose its donors and spending. The Supreme Court acknowledged that multiple factors suggested...

Colorado–Nebraska water clash heads to US Supreme Court as canal fight intensifies
Marianne Goodland
marianne.goodland@coloradopolitics.com
Updated 9 hours ago
The U.S. Supreme Court on Monday agreed to hear Nebraska’s lawsuit against Colorado over the Perkins County canal, a move that advances a legal dispute likely to take years to resolve. The proposed Perkins County canal would run through land...
PREV
PREVIOUS

Adams County to begin public engagement on comprehensive, transportation, parks plans
Adams County will soon initiate its first round of public comments on a trio of long-range planning documents under the collective banner of “Advancing Adams.” Beginning in August, the county began to create a comprehensive plan, a transportation and mobility plan, and updates to the parks, open space & trails plan. “To do this successfully, […]

DA race in 18th Judicial District heads to recount
The race for the top prosecutor spot in the 18th Judicial District will go to a recount, which will start Dec. 1, according to Democratic candidate Amy Padden’s campaign. According to an email from Padden’s campaign, Republican candidate John Kellner leads Padden by 1,433 votes. A vote margin equaling 0.5% or less of the apparent […]