

Colorado’s overdose rates for teens and young people have skyrocketed

Bradyn Heit was a month from his 18th birthday and his high school graduation when he fatally overdosed on fentanyl pills in July 2017.
His mother’s golden child, he’d wanted to play professional football. His mother also had struggled with substances. She died a month after Bradyn.
The teenager who had apparently given Bradyn the pills overdosed 10 months later. A Facebook page used to document his recovery from a car accident became a memorial. Comments of encouragement became remembrances.
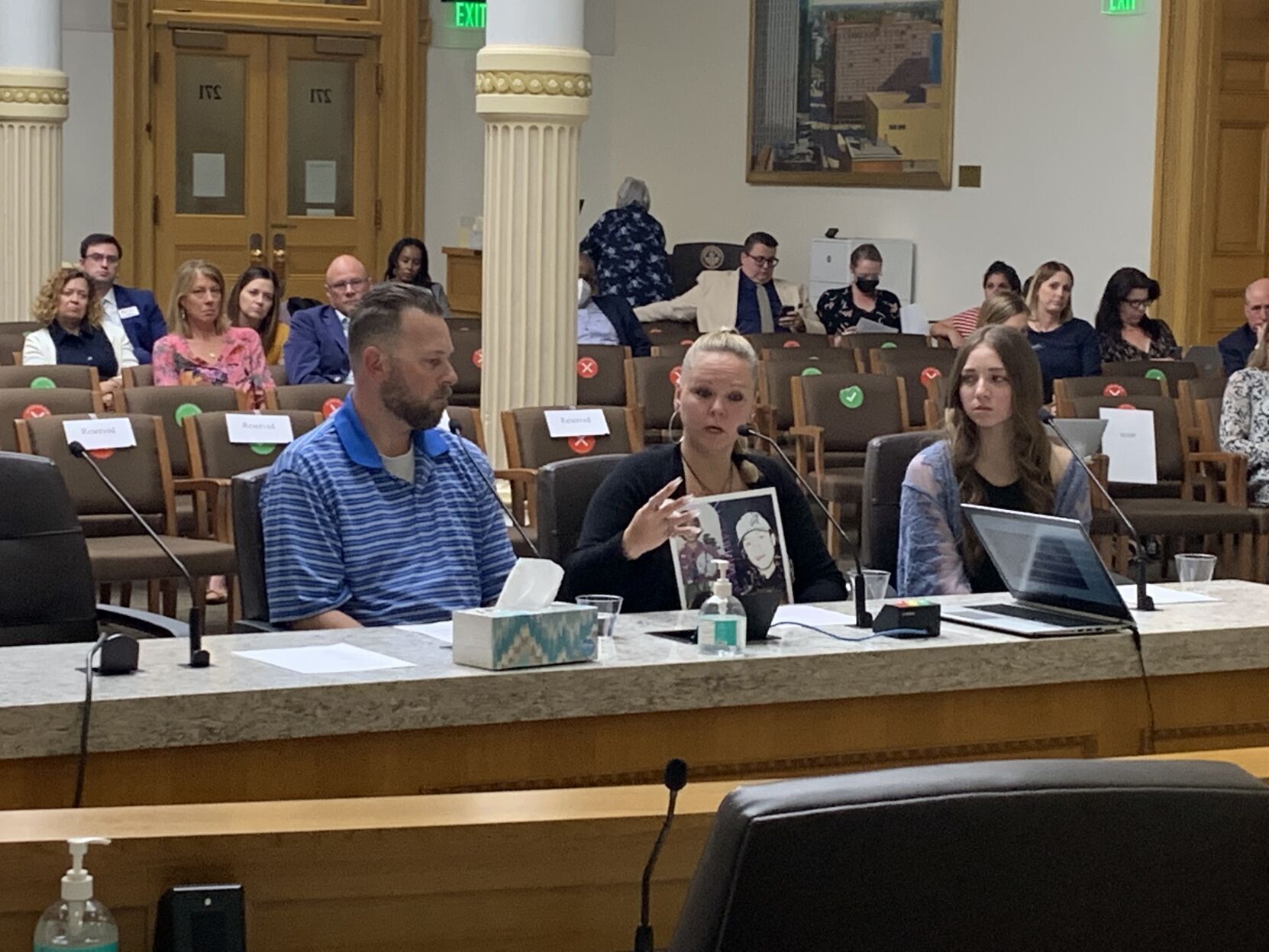
Keith Davidson (an assumed last name for security reasons) was 20, newly out of jail in Weld County and desperately in search of treatment when he overdosed on fentanyl pills in March 2021. His girlfriend, Yesi Chavez, died three months later, at age 21.
Matt Riviere’s two sons, 19-year-old Stephen and 21-year-old Andrew, died on the same night last July, 10 days after Yesi. Riviere told The Gazette in February that his sons were the best of friends and worst of enemies growing up; brothers, in other words.
The view from the streets: A former Colorado drug dealer tells his story
They died together in the bedroom of their apartment after taking what they thought were OxyContin pills.
Chris Thurstone runs Denver Health’s behavioral health services, and he’s the director of the hospital’s adolescent use program. He’s lost five patients to overdoses in his 20-year career. Three of those have died in the past 15 months.
All used fentanyl. All had been in recovery. All relapsed.
As fentanyl has come to dominate the drug supply, it has fueled spiraling overdose rates across the state. But those increases have been sharpest among younger people since fentanyl arrived in force in 2018. In Colorado, total overdoses quintupled for kids ages 10-18 from 2018 to 2021. Rates for 19- to 24-year-olds more than doubled.
Buried in Colorado’s fentanyl bill debate, 3 small tweaks with major importance
While available data indicates young people aren’t using drugs more frequently now than previous generations, the drug that’s predominantly available, fentanyl, is increasing the risk for those who take it, knowingly or otherwise.
Nationwide, “drug overdose and poisoning increased by 83.6% from 2019 to 2020 among children and adolescents, becoming the third-leading cause of death in that age group,” according to a letter published in the New England Journal of Medicine last month.
Fentanyl, coupled with the pandemic and a pre-COVID mental health crisis among youth, are fueling overdoses here, experts said. Poor access to treatment in Colorado – one provider called it “abysmal” – further exacerbates the situation.
“We don’t have enough clinical capacity for those kids,” said Paula Riggs, the director of the Division of Addiction Science, Prevention and Treatment at the University of Colorado School of Medicine. “The ones in treatment are 10% or less (of those who need it).”
The pandemic, and the stressors it brought, are a key piece in understanding increasing youth overdoses, as is fentanyl. But so, too, is the mental health crisis that predated COVID-19’s arrival and has worsened markedly since, several providers said.
Sam Wang, a medical toxicologist and pediatric emergency medicine doctor at Children’s Hospital Colorado, said behavioral health visits to Children’s ER have jumped 41% through the first three months of 2022 compared to last year. Isolation and disruption accelerated the youth mental health emergency, he said, and access to behavioral health treatment overall, not just for substance use, is poor.
Kent MacLennan, the executive director of Rise Above Colorado, said that more teens reported significant mental health challenges between 2018 and 2020, according to his organization’s own data. That doesn’t take into account pandemic impacts, he said, which will almost certainly have worsened the situation.
Just as national reporting has indicated, MacLennan said overall substance use among youth has stayed flat. Overdoses are rising, he and others said, because of fentanyl’s potency and ubiquity. He said Rise Above Colorado is working on a survey of youth now, and the organization is asking adolescents about their risk assessment of fentanyl and of pills from the street.
Increasing the awareness of that risk, he continued, is key in addressing the crisis among teenagers.
“In certain situations, yes, there’s been some good harm-reduction tactics around test strips and awareness,” MacLennan said. “But for those that maybe were looking for (MDMA) as a party drug and have no idea where it’s coming from, we really want to understand what is the level of awareness.”
Though unwitting fentanyl use is significant, Thurstone said all of his current patients knowingly use fentanyl. Some started with it, and others progressed there after taking other opioids.
Substance use is particularly damaging in young people, for whom the brain has not fully developed. Adolescents are more vulnerable to addiction than adults, Thurstone said, and opioids affect brain development. Social development also will be affected by early substance use.
When the pandemic began two years ago, fentanyl had fully found its footing in the Colorado drug supply. It has largely replaced heroin as the dominant opioid on the street, and it’s increasingly being mixed into other drugs, from meth and cocaine to pills masquerading as Xanax, Adderall or OxyContin.
The impact of its increased prevalence has been profound and brutal: In 2017, when Bradyn died, fewer than five people under age 18 fatally overdosed on the substance. Four years later, when Keith died, 35 adolescents died after ingesting fentanyl, out of 46 total overdoses statewide for that age group.
Brian Besser, the special agent in charge of the Drug Enforcement Administration office in Denver, said fentanyl can be purchased via social media apps like Snapchat or Instagram and shipped through the mail. People may know they’re buying fentanyl or may be unaware of the true nature of what they’ve purchased.
If buying the drug is easy, kicking a dependency to it is not. Access to substance-use treatment for youth in Colorado is “abysmal,” Riggs said. She and Thurstone said only 10% of adolescents here who need treatment get it. If 90% of cancer patients couldn’t get the treatment they needed, Riggs said, “we’d be up in arms.” Too often, they and others said, treatment for juveniles only becomes available after kids have been arrested and care is court-ordered.
According to data from the Substance Abuse and Mental Health Services Administration, the proportion of Colorado teenagers who needed treatment for illicit drug use at a specialty facility but couldn’t get it increased from 2015 to 2020, when it was the fifth-worst in the U.S.
Over those same years, the proportion of Colorado teens with substance-use disorders also ticked upward.
Distributing naloxone, which can reverse opioid overdoses, or test strips to check to see if fentanyl is present in a substance, is important, Riggs said, “but the problem is, that’s not treatment.
“At the end of the day, you reverse an overdose, they still have an opioid-use disorder. Treatment is the definitive way we address it.”
Fentanyl is trickier to treat than heroin, morphine or prescription opioids, providers said. It sticks around for longer in a user’s fat tissue, and using vital medications like buprenorphine – which helps treat withdrawal symptoms and curb cravings – requires more attention and a longer bout of abstinence by the user.
Methadone works better, providers said, but it’s more heavily regulated by the federal government, and it has tight controls on when it can be used in juveniles.
Thurstone said patients need to be in moderate to severe withdrawal before they can be given buprenorphine, which, along with its sister medicines, is considered a gold-standard approach to treating opioid use. But that requires patients to be acutely ill – providers have described opioid withdrawal as the flu times 1,000.
What’s more, there are no inpatient detox facilities in the state, Thurstone and Riggs said. While an adult could check into a hospital for a few days to stabilize before starting medication treatment, that option is not available to younger people.
Riggs described a patient, referred to her by Children’s, who was in the emergency room for fentanyl withdrawal. He had been in the ER two weeks before, too, for the same reason. He’d called a list of detox programs and none would let him in because he was 17. He didn’t want to be discharged again. He didn’t want to keep using fentanyl.
His provider wasn’t licensed to write a prescription for buprenorphine. Riggs called another provider who got him started.
She’s started microdosing patients with buprenorphine – necessary because of its effects on a fentanyl user – and slowly increasing their dosages.
“I would say 95% of the youth I see with fentanyl addiction would benefit from an inpatient withdrawal management program to get them stabilized with medication, therapy, resources and then discharge,” Thurstone said.
Denver Health is launching a program of its own, Thurstone added, but it won’t be able to accept its first patient until December 2023. It’ll take that long to jump through the many required hoops.
The detox problem is emblematic of the poor treatment availability for juveniles statewide, providers said. There are too few substance-use providers, and many physicians still don’t the extra training needed to write prescriptions for buprenorphine.
Riggs, who has a federal grant to expand access to an outpatient substance-use clinic at the university, said more clinical capacity is needed across the state. Providers, from primary care doctors to ER physicians, need to work together to hand kids off to substance-use treatment. Don’t give them a list or a number to call, she said. When providers call her, they get approval from the patient to share the patient’s phone number with Riggs. She’ll call them herself, for an initial conversation and evaluation.
“There’s no connective tissue between these systems,” she said, referring to other parts of the medical system and providers like her.
“We’re trying to get better as a health care system as a whole,” Wang, the Children’s physician, said. “But overall, our resources for these kids perhaps aren’t as robust as they should be.”
Denver Health launched an intensive, outpatient treatment program for adolescents last month. Thurstone figured it would take six months to get the word out and start filling spots. Instead, it’s already nearly full. He advocated for school-based treatment: Denver Health has eight substance-use therapists in school health centers.
Now, he said, at least some kids don’t have to be arrested before they get access to treatment.

Homeless recruits of ‘The Program’ say they were told to sign NDAs amid investigations in Colorado
David Migoya
david.migoya@gazette.com
Updated 16 hours ago
Several formerly homeless people — each drawn into an Aurora-based enterprise known as “The Program” that promised free housing and cash in return for letting a home-health business administer prescriptions they were given — said they were pressed into signing...
Homeless recruits of ‘The Program’ say they were told to sign NDAs amid investigations in Colorado
David Migoya
david.migoya@gazette.com
Updated 16 hours ago
Several formerly homeless people — each drawn into an Aurora-based enterprise known as “The Program” that promised free housing and cash in return for letting a home-health business administer prescriptions they were given — said they were pressed into signing...

Trump’s 10th Circuit nominee declines to name 2020 election winner, defends immigration decisions
Michael Karlik
michael.karlik@coloradopolitics.com
Updated 2 hours ago
President Donald Trump’s nominee to the Denver-based federal appeals court declined to say who won the 2020 presidential election during his appearance before the U.S. Senate Judiciary Committee on Wednesday, and defended his recent rulings in immigration detention cases. U.S....

Colorado repeals attorney immigration attestation law after one year
Nico Brambila
nico.brambila@denvergazette.com
Updated 15 hours ago
One year and 12 days. That’s how long a Colorado law requiring attorneys to certify they would not use court data for federal immigration enforcement remained on the books before lawmakers repealed it. Gov. Jared Polis signed the initial legislation,...
Colorado’s ‘right to natural gas’ measure submits signatures to qualify for November ballot
Marissa Ventrelli
marissa.ventrelli@coloradopolitics.com
Updated 18 hours ago
A natural-gas rights initiative backed by Advance Colorado is likely headed to the November ballot, triggering a parallel campaign by environmental groups seeking to impose new liabilities on oil and gas operators. Petitions for Initiative No. 177 were turned in...

Economists: Colorado budget improves slightly, but deficits still loom
Marianne Goodland
marianne.goodland@coloradopolitics.com
Updated 18 hours ago
State economists reported a stronger-than-expected bump in general fund revenue driven largely by higher individual income tax collections, yet warned that Colorado remains on track to begin the next fiscal year with a sizable shortfall. State economists upgraded “significantly” the...

Colorado law allowing lawsuits against ‘conversion therapy’ providers takes effect July 1
Marissa Ventrelli
marissa.ventrelli@coloradopolitics.com
Updated 18 hours ago
With a new law taking effect July 1, Colorado is creating a legal pathway for people to sue licensed providers of “conversion therapy,” even as debate over the practice’s constitutionality continues in the wake of a recent U.S. Supreme Court...
Colorado justices expand ability for civil defendants to avoid participating, win after trial
Michael Karlik
michael.karlik@coloradopolitics.com
Updated 2 hours ago
The Colorado Supreme Court decided on Tuesday that a civil defendant, whose non-participation in the case meant that he legally admitted to the sexual assault allegations against him, could nonetheless prevail after he showed up to testify at trial. A...

Trump heads to Senate as GOP grows more willing to challenge White House
Naomi Lim
naomi-lim@coloradopolitics.com
Updated 21 hours ago
President Donald Trump normally summons congressional Republicans to the White House, but on Wednesday, he is making a rare trip to Capitol Hill to have lunch with GOP senators. And at least publicly, there is one agenda item. “We’re just...

Trump blasts oil companies for not lowering prices to consumers, accuses them of price gouging
Washington Examiner Staff
washington-examiner-staff@coloradopolitics.com
Updated 21 hours ago
President Donald Trump criticized “big oil companies” for not lowering prices for consumers, even though oil purchase costs have dropped. He accused oil companies of price gouging consumers, ordered the Department of Justice to investigate current practices, and demanded that...
PREV
PREVIOUS

OUT WEST ROUNDUP | Wildlife officials agree on Canada lynx protections in western states
MONTANA Canada lynx protections deal sealed by US, environmentalists BILLINGS – U.S. wildlife officials have agreed to craft a new habitat plan for the snow-loving Canada lynx that could include more land in western states where the rare animals would be protected, according to a legal agreement made public on April 26. The U.S. Fish […]

Denver expects to meet its revenue goal from increased parking meter rates
Denver has more than doubled its revenue from downtown parking meters in the first quarter since doubling the cost from $1 to $2 an hour, according to new figures released by the city. From January through March, Denver generated $3,775,066 in revenue from parking meter fees, while during the same period in 2021 the city generated […]